
Impact of Dietitian-Led Nutrition Therapy of Food Order on 5-Year Glycemic Control in Outpatients with Type 2 Diabetes at Primary Care Clinic: Retrospective Cohort Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
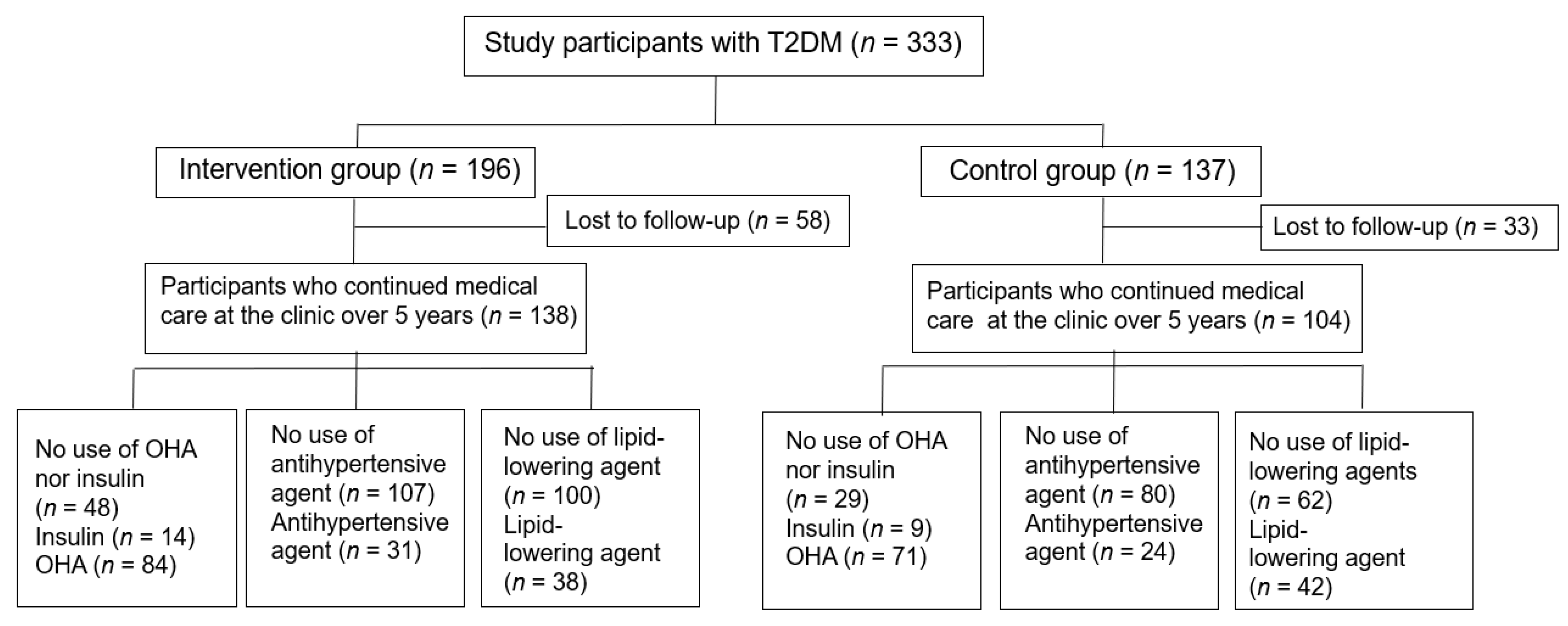
2.1. Patients
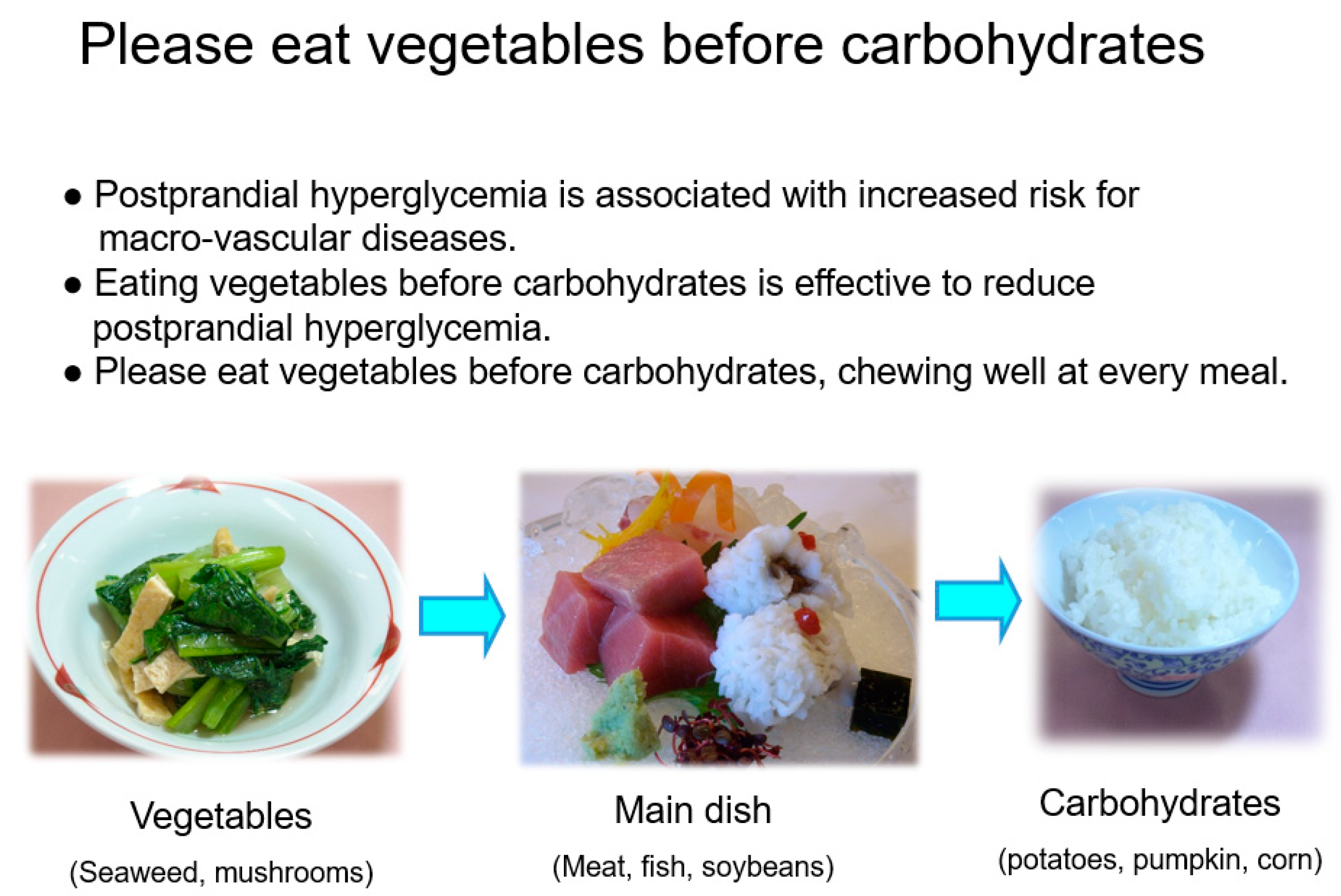
2.2. Dietitian-Led Medical Nutrition Therapy of Food Order in the Intervention Group
2.3. Laboratory Analyses
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Study Patients
3.2. Effects of Long-Term Glycemic Control, Blood Pressure, and Lipid Profile
3.3. Changes in Nutritional Intake
3.4. Changes in Diabetic Complications, Hypertension, Dyslipidemia, and Macro-Vascular Complications
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nathan, D.M. Long-term complications of diabetes mellitus. N. Engl. J. Med. 1993, 328, 1676–1685. [Google Scholar] [CrossRef]
- Diabetes Control and Complications Trial Research Group; Nathan, D.M.; Genuth, S.; Lachin, J.; Cleary, P.; Crofford, O.; Davis, M.; Rand, L.; Siebert, C. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar] [CrossRef]
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998, 352, 837–853. [Google Scholar] [CrossRef]
- Delahantry, L.; Simkins, S.W.; Camelon, K. Expanded role of the dietitian in the diabetes Control and Complications Trial: Implications for clinical practice. The DCCT Research Group. Am. Diet. Assoc. 1993, 93, 758–764. [Google Scholar] [CrossRef]
- Bloomgarden, Z.T.; Karmally, W.; Metzger, M.J.; Brothers, M.; Nechemias, C.; Bookman, J.; Faierman, D.; Ginsberg-Fellner, F.; Rayfield, E.; Brown, W.V. Randomised, controlled trial of diabetic patient education: Improved knowledge without improved metabolic status. Diabetes Care 1987, 10, 263–272. [Google Scholar] [CrossRef]
- Pastors, J.G.; Warshaw, H.; Daly, A.; Franz, M.; Kulkarni, K. The evidence for the effectiveness of medical nutrition therapy in diabetes management. Diabetes Care 2002, 25, 608–613. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association. 5 facilitating behavior change and well-being to improve health outcomes: Standards of medical care in diabetes-2021. Diabetes Care 2021, 44, S53–S72. [Google Scholar] [CrossRef]
- Clement, S. Diabetes self-management education. Diabetes Care 1995, 18, 1204–1214. [Google Scholar] [CrossRef] [Green Version]
- Guideline for Diabetes Treatment 2020–2021; Japan Diabetes Society: Tokyo, Japan, 2020; pp. 48–51.
- Sato, Y.; Sone, H.; Kobayashi, M.; Kawamori, R.; Atsumi, Y.; Oshida, Y.; Tanaka, S.; Suzuki, S.; Makita, S.; Ohsawa, I.; et al. Current Situation of Exercise Therapy in Patients With Diabetes Mellitus in Japan (Report No. 2): A Nationwide Survey to Patients Using the Questionnaires. Jpn. Diab. Soc. 2015, 58, 850–859. [Google Scholar]
- Imai, S.; Fukui, M.; Ozasa, N.; Ozeki, T.; Kurokawa, M.; Komatsu, T.; Kajiyama, S. Eating vegetables before carbohydrates improves postprandial glucose excursions. Diabet. Med. 2013, 30, 370–372. [Google Scholar] [CrossRef] [Green Version]
- Imai, S.; Matsuda, M.; Togawa, C.; Oyabu, K.; Kajiyama, S. Effect of Eating Vegetables before Carbohydrates’ on Glycaemic Control in Japanese Outpatients with Type 2 Diabetes. J. Jpn. Diet. Assoc. 2010, 53, 1084–1091. [Google Scholar]
- Haneda, M.; Utsunomiya, K.; Koya, D.; Babazono, T.; Moriya, T.; Makino, H.; Kimura, K.; Suzuki, Y.; Wada, T.; Ogawa, S.; et al. A new Classification of Diabetic Nephropathy 2014: A report from Joint Committee on Diabetic Nephropathy. J. Diabetes Investig. 2015, 6, 242–246. [Google Scholar] [CrossRef]
- Araki, E.; Goto, A.; Kondo, T.; Noda, M.; Noto, H.; Origasa, H.; Osawa, H.; Taguchi, A.; Tanizawa, Y.; Tobe, K.; et al. Japanese Clinical Practice Guideline for Diabetes 2019. J. Diabetes Investig. 2020, 11, 1020–1076. [Google Scholar] [CrossRef]
- Imai, S.; Fukui, M.; Kajiyama, S. Effect of eating vegetables before carbohydrates on glucose excursions in patients with type 2 diabetes. J. Clin. Biochem. Nutr. 2014, 54, 7–11. [Google Scholar] [CrossRef] [Green Version]
- Ceriello, A. The post-prandial state and cardiovascular disease: Relevance to diabetes mellitus. Diabetes Metab. Res. Rev. 2000, 16, 125–132. [Google Scholar] [CrossRef]
- Fujishima, M.; Kiyohara, Y.; Kato, I.; Ohmura, T.; Iwamoto, H.; Nakayama, K.; Ohmori, S.; Yoshitake, T. Diabetes and cardiovascular disease in a prospective population survey in Japan: The Hisayama study. Diabetes 1996, 45, S14–S16. [Google Scholar] [CrossRef]
- Su, G.; Mi, S.H.; Tao, H.; Li, Z.; Yang, H.X.; Zheng, H.; Zhou, Y.; Tian, L. Impact of Admission Glycaemic Variability, Glucose, and Glycosylated Hemoglobin on Major Adverse Cardiac Events After Acute Myocardial Infarction Variability. Diabetes Care 2013, 36, 1026–1032. [Google Scholar] [CrossRef] [Green Version]
- Tuomilehto, J.; Lindström, J.; Eriksson, J.G.; Valle, T.T.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Laakso, M.; Louheranta, A.; Rastas, M.; et al. Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N. Engl. J. Med. 2001, 344, 1343–1350. [Google Scholar] [CrossRef]
- American Diabetes Association. Economic costs of diabetes in the U.S. in 2017. Diabetes Care 2018, 41, 917–928. [Google Scholar] [CrossRef] [Green Version]
- Huang, M.C.; Hsu, C.C.; Wang, H.S.; Shin, S.J. Prospective randomized controlled trial to evaluate effectiveness of registered dietitian-led diabetes management on glycaemic and diet control in a primary care setting in Taiwan. Diabetes Care 2010, 33, 233–239. [Google Scholar] [CrossRef] [Green Version]
- Beresford, S.A.; Curry, S.J.; Kristal, A.R.; Lazovich, D.; Feng, Z.; Wagner, E.H. A dietary intervention in primary care practice: The Eating Patterns Study. Am. J. Public Health 1997, 87, 610–616. [Google Scholar] [CrossRef] [Green Version]
- Peyrot, M.; Rubin, R.R.; Lauritzen, T.; Snoek, F.J.; Matthews, D.R.; Skovlund, S.E. Psychosocial problems and barriers to improved diabetes management: Results of the Cross-National Diabetes Attitudes, Wishes and Needs (DAWN) Study. Diabet. Med. 2005, 22, 1379–1385. [Google Scholar] [CrossRef]
- Snoek, F.J. Barriers to good glycaemic control: The patient’s perspective. Int. J. Obes. 2000, 24, S12–S20. [Google Scholar] [CrossRef] [Green Version]
- American Diabetes Association; Bantle, J.P.; Wylie-Rosett, J.; Albright, A.L.; Apovian, C.M.; Clark, N.G. Nutrition recommendations and interventions for diabetes: A position statement of the American Diabetes Association. Diabetes Care 2008, 31, S61–S78. [Google Scholar] [CrossRef] [Green Version]
- Imai, S.; Matsuda, M.; Hasegawa, G.; Fukui, M.; Obayashi, H.; Ozasa, N.; Kajiyama, S. A simple meal plan of ‘eating vegetables before carbohydrate’ was more effective for achieving glycaemic control than an exchange–based meal plan in Japanese patients with type 2 diabetes. Asia Pac. J. Clin. Nutr. 2011, 20, 161–168. [Google Scholar]
- Imai, S.; Matsuda, M.; Miyatani, S.; Hasegawa, G.; Fukui, M.; Kajiyama, S. Crossover Study of the Effect of “Vegetables Before Carbohydrates” on the Reduction of the Postprandial Glucose and Insulin Levels in Japanese Patients with Type 2 Diabetes Mellitus. J. Jpn. Diabetes Soc. 2010, 53, 112–115. [Google Scholar]
- Jakubowicz, D.; Froy, O.; Ahren, B.; Boaz, M.; Landau, Z.; Bar-Dayan, Y.; Ganz, T.; Barnea, M.; Wainstein, J. Incretin, insulinotropic and glucose-lowering effects of whey protein pre-load in type 2 diabetes: A randomised clinical trial. Diabetologia 2014, 57, 1807–1811. [Google Scholar] [CrossRef]
- Shukla, A.P.; Iliescu, R.G.; Thomas, C.E.; Aronne, L.J. Food Order Has a Significant Impact on Postprandial Glucose and Insulin Levels. Diabetes Care 2015, 38, e98–e99. [Google Scholar] [CrossRef] [Green Version]
- Imai, S.; Fukui, M.; Kajiyama, S. Comment on Shukla et al. Food Order Has a Significant Impact on Postprandial Glucose and Insulin Levels. Diabetes Care 2015, 38, e196. [Google Scholar] [CrossRef] [Green Version]
- Trico, D.; Filice, E.; Trifiro, S.; Natali, A. Manipulating the sequence of food ingestion improves glycemic control in type 2 diabetic patients under free-living conditions. Nutr. Diabetes 2016, 6, e226. [Google Scholar] [CrossRef] [Green Version]
- Shukla, A.P.; Mauer, E.; Igel, L.I.; Truong, W.; Casper, A.; Kumar, R.B.; Saunders, K.H.; Aronne, L.J. Effect of Food Order on Ghrelin Suppression. Diabetes Care 2018, 41, e76–e77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yabe, D.; Kuwata, H.; Fujiwara, Y.; Sakaguchi, M.; Moyama, S.; Makabe, N.; Murotani, K.; Asano, H.; Ito, S.; Mishima, H.; et al. Dietary instructions focusing on meal-sequence and nutritional balance for prediabetes subjects: An exploratory, cluster-randomized, prospective, open-label, clinical trial. J. Diabetes Complicat. 2019, 33, 107450. [Google Scholar] [CrossRef] [PubMed]
- Nesti, L.; Mengozzi, A.; Trico, D. Impact of nutrient type and sequence on glucose tolerance: Physiological insights and therapeutic implications. Front. Endocrinol. 2019, 10, 144. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.M.; Jenkins, D.J. Carbohydrate digestibility and metabolic effects. J. Nutr. 2007, 137, S2539–S2546. [Google Scholar] [CrossRef] [PubMed]
- Howarth, N.C.; Saltzman, E.; Roberts, S.B. Dietary fiber and weight regulation. Nutr. Rev. 2001, 59, 129–139. [Google Scholar] [CrossRef]
- Holt, S.; Heading, R.C.; Carter, D.C.; Prescott, L.F.; Tothill, P. Effect of gel fibre on gastric emptying and absorption of glucose and paracetamol. Lancet 1979, 313, 636–639. [Google Scholar] [CrossRef]
- McIntosh, M.; Miller, C. A diet containing food rich in soluble and insoluble fiber improves glycaemic control and reduces hyperlipidemia among patients with type 2 diabetes mellitus. Nutr. Rev. 2001, 59, 52–55. [Google Scholar] [CrossRef]
- Jenkins, D.J.; Wolever, T.M.; Taylor, R.H.; Barker, H.; Fielden, H.; Baldwin, J.M.; Bowling, A.C.; Newman, H.C.; Jenkins, A.L.; Goff, D.V. Glycaemic index of foods: A physiological basis for carbohydrate exchange. Am. J. Clin. Nutr. 1981, 34, 362–366. [Google Scholar] [CrossRef] [Green Version]
- Kuwata, H.; Iwasaki, M.; Shimizu, S.; Minami, K.; Maeda, H.; Seino, S.; Nakada, K.; Nosaka, C.; Murotani, K.; Kurose, T.; et al. Meal sequence and glucose excursion, gastric emptying and incretin secretion in type 2 diabetes: A randomised, controlled crossover, exploratory trial. Diabetologia 2016, 59, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.G.; Hahn, S.; Oh, T.J.; Kwak, S.H.; Park, K.S.; Cho, Y.M. Differences in the glucose-lowering efficacy of dipeptidyl peptidase-4 inhibitors between Asians and non-Asians: A systematic review and meta-analysis. Diabetologia 2013, 56, 696–708. [Google Scholar] [CrossRef] [Green Version]
- Saito, Y.; Kajiyama, S.; Nitta, A.; Miyawaki, T.; Matsumoto, S.; Ozasa, N.; Kajiyama, S.; Hashimoto, Y.; Fukui, M.; Imai, S. Eating Fast Has a Significant Impact on Glycemic Excursion in Healthy Women: Randomized Controlled Cross-Over Trial. Nutrients. 2020, 12, 2767. [Google Scholar] [CrossRef] [PubMed]
- Livingstone, M.B.; Black, A.E. Markers of the validity of reported energy intake. J. Nutr. 2003, 133 (Suppl. S3), 895S–920S. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Intervention Group (n =138) | Control Group (n = 104) | p | |
|---|---|---|---|
| Male/Female (n) | 62/76 | 59/45 | 0.091 |
| Age (years) | 64.5 ± 11.0 | 66.4 ± 10.2 | 0.169 |
| Duration of diabetes (years) | 7.1 ± 8.2 | 7.8 ± 6.0 | 0.609 |
| Body weight (kg) | 61.3 ± 13.3 | 63.5 ± 12.5 | 0.184 |
| BMI (kg/m2) | 24.0 ± 4.4 | 24.5 ± 3.2 | 0.553 |
| HbA1c (%) (mmol/mol) | 8.5 ± 1.7 (69) | 7.9 ± 1.2 (62) | 0.005 |
| SBP (mmHg) | 132 ± 18 | 133 ± 15 | 0.786 |
| DBP (mmHg) | 75 ± 11 | 73 ± 10 | 0.307 |
| Total-C (mg/dL) | 213 ± 35 | 205 ± 34 | 0.086 |
| LDL-C (mg/dL) | 131 ± 30 | 123 ± 29 | 0.027 |
| HDL-C (mg/dL) | 56 ± 15 | 56 ± 15 | 0.668 |
| TG (mg/dL) | 140 ± 83 | 141 ± 77 | 0.898 |
| Diet only | |||
| No insulin or OHA, n (%) | 48 (35) | 29 (28) | 0.361 |
| No antihypertensive agent, n (%) | 107 (78) | 80 (77) | 1.000 |
| No lipid-lowering agent, n (%) | 100 (72) | 62 (60) | 0.100 |
| Prescribed medicine | |||
| Insulin, n (%) | 14 (10) | 9 (9) | 1.000 |
| OHA, n (%) | 84 (61) | 71 (68) | 0.375 |
| Sulfonylurea, n (%) | 61 (44) | 62 (60) | 0.033 |
| Metformin, n (%) | 18 (13) | 31 (30) | 0.005 |
| α-GI inhibitor, n (%) | 37 (27) | 43 (41) | 0.052 |
| Glinide, n (%) | 3 (2) | 0 (0) | 0.497 |
| Thiazolidinedione, n (%) | 8 (6) | 7 (7) | 1.000 |
| Antihypertensive agent, n (%) | 31 (22) | 24 (23) | 1.000 |
| Lipid-lowering agent, n (%) | 38 (31) | 42 (42) | 0.142 |
| Intervention Group (n = 138) | Control Group (n = 104) | |||||||
|---|---|---|---|---|---|---|---|---|
| Baseline | After 1 Year | After 3 Years | After 5 Years | Baseline | After 1 Year | After 3 Years | After 5 Years | |
| Body weight (kg) | 61.3 ± 13.3 | 61.0 ± 12.6 | 61.6 ± 12.8 | 60.1 ± 14.3 | 63.5 ± 12.0 | 64.6 ± 11.1 | 64.5 ± 10.6 | 63.8 ± 13.3 |
| BMI (kg/m2) | 24.0 ± 4.4 | 23.8 ± 3.9 | 23.9 ± 3.9 | 23.8 ± 4.5 | 24.5 ± 3.2 | 24.5 ± 3.2 | 24.5 ± 3.0 | 24.4 ± 3.4 |
| HbA1c (%) (mmol/mol) | 8.5 ± 1.7 (69) | 7.3 ± 1.0 (56) ***††† | 7.5 ± 1.2(58) ***††† | 7.6 ± 1.1 (59) ***† | 7.9 ± 1.2 (62) †† | 8.4 ± 1.1 (68) * | 8.3 ± 1.0 (67) * | 8.0 ± 1.2 (63) |
| SBP (mmHg) | 132 ± 18 | 125 ± 13 *** | 124 ± 9 *** | 125 ± 11 *** | 133 ± 15 | 126 ± 12 *** | 127 ± 10 *** | 128 ± 17 |
| DBP (mmHg) | 75 ± 11 | 71 ± 9 *** | 71 ± 9 *** | 68 ± 8 ***† | 73 ± 10 | 70 ± 8 ** | 72 ± 7 * | 71 ± 8 |
| Total-C (mg/dL) | 213 ± 35 | 210 ± 35 | 202 ± 33 ** | 198 ± 32 ** | 205 ± 34 | 199 ± 34 † | 197 ± 38 ** | 190 ± 31 *** |
| LDL-C (mg/dL) | 131± 30 | 119 ± 28 *** | 120 ± 30 ** | 120 ±30 * | 123 ± 29 † | 119 ± 24 | 116 ± 26 | 110 ± 28 **† |
| HDL-C (mg/dL) | 56 ± 15 | 57 ± 15 | 58 ± 16 | 56 ± 15 | 56 ± 15 | 56 ± 12 | 56 ± 15 | 57 ± 15 |
| TG (mg/dL) | 140 ± 83 | 131 ± 75 | 129 ± 70 * | 139 ± 82 | 141 ± 77 | 140 ± 87 | 157 ± 117 | 139 ± 73 |
| Baseline | After Intervention | |
|---|---|---|
| A | ||
| Energy (kcal) | 2169 ± 91 | 1626 ± 46 *** |
| Protein (g) | 76.8 ± 2.6 | 68.2 ± 2.0 ** |
| Fat (g) | 64.1 ± 3.7 | 45.4 ± 2.0 *** |
| Carbohydrates (g) | 291 ± 14 | 221 ± 7 *** |
| Cholesterol (mg) | 393 ± 43 | 257 ± 22 ** |
| Dietary fiber (g) | 13.7 ± 0.5 | 16.5 ± 0.7 ** |
| Salt (g) | 11.3 ± 0.3 | 9.1 ± 0.3 *** |
| B | ||
| Grains (g) | 459 ± 22 | 345 ± 16 *** |
| Potatoes (g) | 40.3 ± 6.3 | 47.2 ± 7.3 |
| Green vegetables (g) | 91 ± 9 | 182 ± 15 *** |
| Other vegetables (g) | 155 ± 11 | 221 ± 19 ** |
| Mushrooms (g) | 9.1 ± 2.2 | 12.1 ± 2.7 |
| Seaweed (g) | 5.4 ± 1.3 | 4.1 ± 0.9 |
| Soy and soy products (g) | 66.7 ± 9.4 | 68.9 ± 10.0 |
| Fish (g) | 88.6 ± 7.9 | 96.9 ± 8.2 |
| Meats (g) | 76.3 ± 8.7 | 61.2 ± 7.6 * |
| Eggs (g) | 38.2 ± 3.9 | 27.6 ± 3.5 * |
| Daily products (g) | 79.6 ± 12.3 | 85.0 ± 11.3 |
| Fruits (g) | 113.4 ± 15.6 | 67.3 ± 12.3 ** |
| Sweetened beverages (g) | 396 ± 44 | 321 ± 41 ** |
| Sugar (g) | 12.4 ± 2.1 | 6.9 ± 1.0 * |
| Sweets and snacks (g) | 31.2 ± 4.9 | 17.6 ± 3.2 * |
| Nuts (g) | 2.4 ± 0.7 | 2.0 ± 0.6 |
| Oil (g) | 16.8 ± 1.6 | 10.4 ± 1.1 ** |
| Intervention Group (n =138) | Control Group (n = 104) | |||
|---|---|---|---|---|
| Baseline | After 5 Years | Baseline | After 5 Years | |
| Diabetic nephropathy, n (%) | 2 (1) | 4 (3) | 6 (6) | 10 (10) |
| Diabetic neuropathy, n (%) | 6 (4) | 18 (13) * | 4 (4) | 17 (16) ** |
| Arteriosclerosis, n (%) | 56 (41) | 59 (41) | 39 (38) | 64 (62) **†† |
| Coronary heart disease, n (%) | 12 (9) | 14 (10) | 10 (10) | 17 (16) |
| Cerebrovascular disease, n (%) | 16 (12) | 21 (15) | 12 (12) | 23 (22) |
| Hypertension, n (%) | 39 (28) | 40 (29) | 32 (31) | 44 (42) |
| Dyslipidemia, n (%) | 49 (36) | 49 (36) | 56 (54) † | 71 (68) ††† |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nitta, A.; Imai, S.; Kajiayama, S.; Matsuda, M.; Miyawaki, T.; Matsumoto, S.; Kajiyama, S.; Hashimoto, Y.; Ozasa, N.; Fukui, M. Impact of Dietitian-Led Nutrition Therapy of Food Order on 5-Year Glycemic Control in Outpatients with Type 2 Diabetes at Primary Care Clinic: Retrospective Cohort Study. Nutrients 2022, 14, 2865. https://doi.org/10.3390/nu14142865
Nitta A, Imai S, Kajiayama S, Matsuda M, Miyawaki T, Matsumoto S, Kajiyama S, Hashimoto Y, Ozasa N, Fukui M. Impact of Dietitian-Led Nutrition Therapy of Food Order on 5-Year Glycemic Control in Outpatients with Type 2 Diabetes at Primary Care Clinic: Retrospective Cohort Study. Nutrients. 2022; 14(14):2865. https://doi.org/10.3390/nu14142865
Chicago/Turabian StyleNitta, Ayasa, Saeko Imai, Shizuo Kajiayama, Mikuko Matsuda, Takashi Miyawaki, Shinya Matsumoto, Shintaro Kajiyama, Yoshitaka Hashimoto, Neiko Ozasa, and Michiaki Fukui. 2022. "Impact of Dietitian-Led Nutrition Therapy of Food Order on 5-Year Glycemic Control in Outpatients with Type 2 Diabetes at Primary Care Clinic: Retrospective Cohort Study" Nutrients 14, no. 14: 2865. https://doi.org/10.3390/nu14142865