Knowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant Patients



Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Knowledge and Attitudes Towards Periodontal Disease
3.2. Attitudes and Practice Behaviour
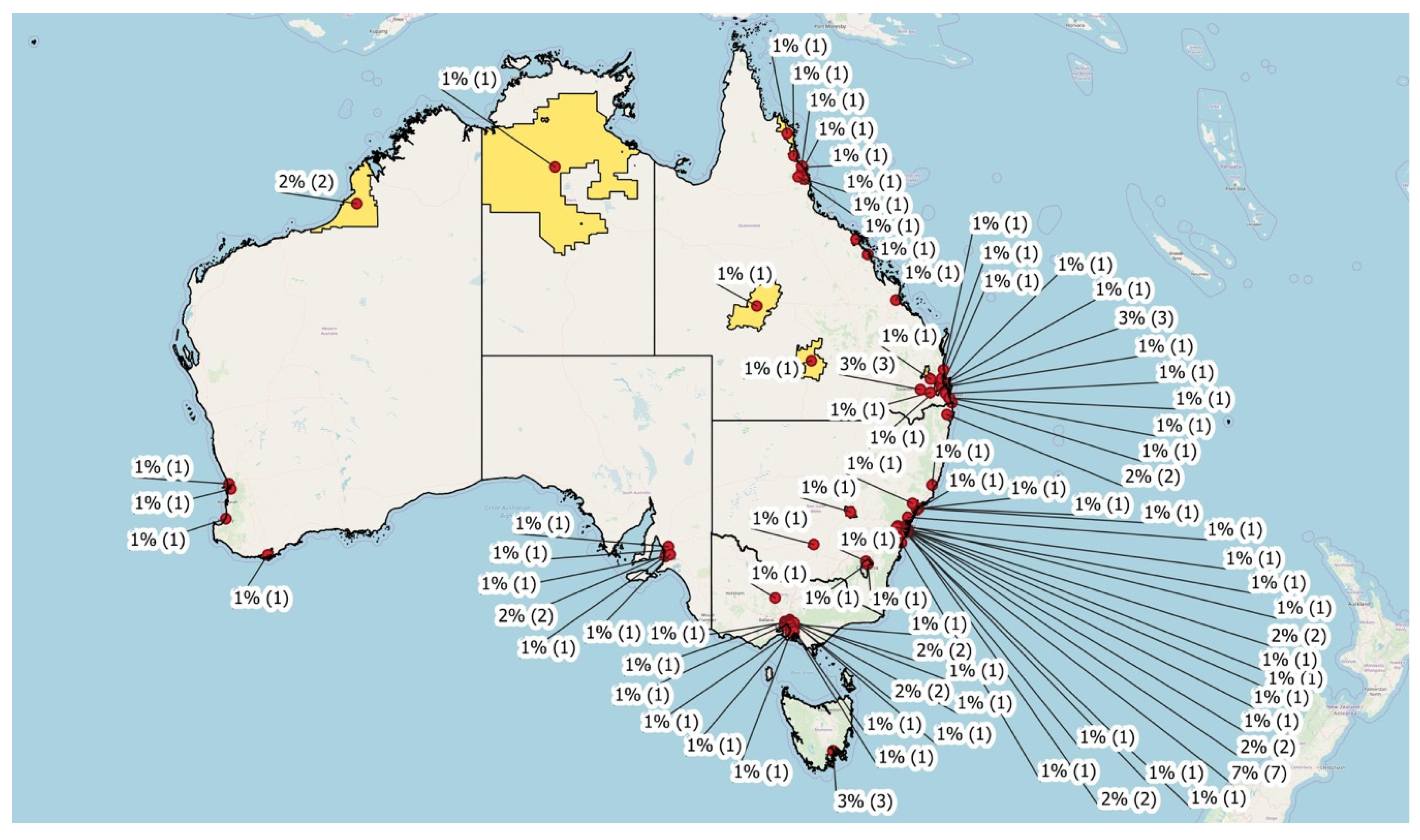
3.3. Midwives and Practice Location
4. Discussion
4.1. Attitudes and Practice Behaviour
4.2. Differences in Practice Location
4.3. Limitations
4.4. Future Directions
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
- How would you classify periodontal diseases?
- a.
- Auto-immune disorder
- b.
- Inflammation and bacterial infection
- c.
- Degenerative process
- d.
- Osteoporosis
- e.
- Metastatic process
- Which clinical signs are associated with periodontal diseases?
- a.
- Caries
- b.
- Tooth mobility
- c.
- Gingival bleeding
- d.
- Alveolar bone destruction
- e.
- Tooth loss
- In your opinion, which risk factors contribute to gum disease initiation? (Choose maximum 4 answers)
- a.
- Tooth decay
- b.
- Excessive sugar consumption
- c.
- Genetics
- d.
- Smoking
- e.
- Dental plaque
- f.
- Pregnancy
- g.
- Poor oral hygiene
- In your opinion, which risk factors contribute to gum disease progression? (Choose maximum 4 answers)
- a.
- Tooth decay
- b.
- Excessive sugar consumption
- c.
- Genetics
- d.
- Smoking
- e.
- Dental plaque
- f.
- Pregnancy
- g.
- Poor oral hygiene
- Which oral signs are often observed related to pregnancy?
- a.
- Gingival overgrowth
- b.
- Gingival bleeding
- c.
- Caries
- d.
- Tooth loss
- Do periodontal diseases influence pregnancy outcomes?
- a.
- No
- b.
- Yes – Increased incidence of low genital-tract infection
- c.
- Yes – Increased incidence of pre-eclampsia
- d.
- Yes – Increased incidence of preterm birth
- e.
- Yes – Increased incidence of low-weight newborn
- f.
- Yes – Increased incidence of spontaneous abortion
- Are periodontal diseases preventable during pregnancy?
- a.
- No – They’re an expected side effect during pregnancy.
- b.
- Yes – They can be prevented or arrested during pregnancy.
- Periodontal diseases can be prevented by:
- a.
- Using fluoridated toothpaste
- b.
- Using dental floss or interdental brushes
- c.
- Effective tooth-brushing technique
- d.
- Control of psychological stress
- e.
- Smoking cessation
- For patients with periodontal disease, periodontal treatment is beneficial for improving oral health.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- Periodontal disease can have an adverse effect on pregnancy outcomes.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- Treatment of periodontal disease during pregnancy positively affects pregnancy outcomes.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- Asking pregnant patients about their oral health is outside the routine practices of a midwife.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- Conducting an examination of the oral cavity during pregnancy is outside the routine practices of a midwife
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- It is important for a pregnant woman to receive routine dental care during her pregnancy.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- There is not sufficient time to address oral health during a care visit with a midwife.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- I am up to date on the topic of oral health and pregnancy.
- a.
- Strongly agree, Agree, Neutral, Disagree, Strongly disagree
- I routinely ask questions related to oral health during consultation with pregnant patients.
- a.
- Yes, No
- I routinely perform a visual oral examination during consultation with pregnant patients.
- a.
- Yes, No
- I provide oral health-related information during consultation with pregnant patients.
- a.
- Routinely
- b.
- If patient is considered at risk
- c.
- Never
- I refer patients to their dentist for a check-up.
- a.
- Routinely
- b.
- If patient is considered at risk
- c.
- Never
- Participant’s Sex: Male, Female, Other
- Participant’s Age: (years)
- How long have you practiced as a midwife?
- a.
- Current Midwifery student
- b.
- ≤10 years
- c.
- 10–20 years
- d.
- 21–30 years
- e.
- 31–40 years
- f.
- 40+ years
- What is your current occupation?
- a.
- Currently practicing in Australia
- b.
- Retired midwife
- c.
- Current midwifery student
- d.
- Unemployed
- Midwifery practice location: (Postal code)
- Midwifery practice location:
- a.
- Urban
- b.
- Rural
- Midwifery practice setting
- a.
- Hospital
- b.
- Private practice
- c.
- Hospital and private practice
- How would you rate your oral health?
- a.
- Excellent
- b.
- Good
- c.
- Neutral
- d.
- Poor
- e.
- Very poor
- On average, how often do you visit the dentist?
- a.
- Every 6 months
- b.
- Every 12 months
- c.
- Every 12–18 months
- d.
- Only if in pain
- e.
- Never
- Have you ever been diagnosed with periodontal disease? Yes/No
- Have you ever been diagnosed with periodontal disease and received treatment for this condition? Yes/No
Appendix B

References
- Zekeridou, A.; Mombelli, A.; Cancela, J.; Courvoisier, D.; Giannopoulou, C. Systemic inflammatory burden and local inflammation in periodontitis: What is the link between inflammatory biomarkers in serum and gingival crevicular fluid? Clin. Exp. Dent. Res. 2019, 5, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Borgnakke, W.S.; Ylöstalo, P.V.; Taylor, G.W.; Genco, R.J. Effect of periodontal disease on diabetes: Systematic review of epidemiologic observational evidence. J. Periodontol. 2013, 84, 135–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cardoso, E.M.; Reis, C.; Manzanares-Céspedes, M.C. Chronic periodontitis, inflammatory cytokines, and interrelationship with other chronic diseases. Postgrad. Med. 2018, 130, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Liccardo, D.; Cannavo, A.; Spagnuolo, G.; Ferrara, N.; Cittadini, A.; Rengo, C.; Rengo, G. Periodontal Disease: A Risk Factor for Diabetes and Cardiovascular Disease. IJMS 2019, 20, 1414. [Google Scholar] [CrossRef] [Green Version]
- Kuo, L.-C.; Polson, A.M.; Kang, T. Associations between periodontal diseases and systemic diseases: A review of the inter-relationships and interactions with diabetes, respiratory diseases, cardiovascular diseases and osteoporosis. Public Health 2008, 122, 417–433. [Google Scholar] [CrossRef]
- Winning, L.; Patterson, C.C.; Cullen, K.M.; Kee, F.; Linden, G.J. Chronic periodontitis and reduced respiratory function. J. Clin. Periodontol. 2019, 46, 266–275. [Google Scholar] [CrossRef]
- Preventing Periodontal Disease; American Academy of Periodontology: Chicago, IL, USA, 2019; Available online: https://www.perio.org/consumer/prevent-gum-disease (accessed on 18 February 2020).
- Wu, M.; Chen, S.-W.; Jiang, S.-Y. Relationship between Gingival Inflammation and Pregnancy. Mediat. Inflamm. 2015, 2015, 1–11. [Google Scholar] [CrossRef]
- Silk, H.; Douglass, A.B.; Douglass, J.M.; Silk, L. Oral Health During Pregnancy. Am. Fam. Physician 2008, 77, 1139–1144. [Google Scholar]
- Kruse, A.B.; Kuerschner, A.C.; Kunze, M.; Woelber, J.P.; Al-Ahmad, A.; Wittmer, A.; Vach, K.; Ratka-Krueger, P. Association between high risk for preterm birth and changes in gingiva parameters during pregnancy—A prospective cohort study. Clin. Oral Investig. 2018, 22, 1263–1271. [Google Scholar] [CrossRef]
- Reyes, L.; Phillips, P.; Wolfe, B.; Golos, T.G.; Walkenhorst, M.; Progulske-Fox, A.; Brown, M. Porphyromonas gingivalis and adverse pregnancy outcome. J. Oral Microbiol. 2017, 9, 1374153. [Google Scholar] [CrossRef] [Green Version]
- Dasanayake, A.P.; Gennaro, S.; Hendricks-Muñoz, K.D.; Chhun, N. Maternal Periodontal Disease, Pregnancy, and Neonatal Outcomes. MCN Am. J. Matern./Child Nurs. 2008, 33, 45–49. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.L.; Mayberry, L.J. Pregnancy and Oral Health: A Review and Recommendations to Reduce Gaps in Practice and Research. MCN Am. J. Matern./Child Nurs. 2008, 33, 32–37. [Google Scholar] [CrossRef]
- Morgan, M.A.; Crall, J.; Goldenberg, R.L.; Schulkin, J. Oral health during pregnancy. J. Matern.-Fetal Neonatal Med. 2009, 22, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Iheozor-Ejiofor, Z.; Middleton, P.; Esposito, M.; Glenny, A.-M. Treating periodontal disease for preventing adverse birth outcomes in pregnant women. Cochrane Database Syst. Rev. 2017. [Google Scholar] [CrossRef]
- Vanterpool, S.F.; Been, J.V.; Houben, M.L.; Nikkels, P.G.J.; De Krijger, R.R.; Zimmermann, L.J.I.; Kramer, B.W.; Progulske-Fox, A.; Reyes, L. Porphyromonas gingivalis within Placental Villous Mesenchyme and Umbilical Cord Stroma Is Associated with Adverse Pregnancy Outcome. PLoS ONE 2016, 11, e0146157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parthiban, P.S.; Mahendra, J.; Logaranjani, A.; Shanmugam, S.; Balakrishnan, A.; Junaid, M.; Namasivayam, A. Association between specific periodontal pathogens, Toll-like receptor-4, and nuclear factor-κB expression in placental tissues of pre-eclamptic women with periodontitis. J. Investig. Clin. Dent. 2018, 9, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Meqa, K.; Dragidella, F.; Disha, M.; Sllamniku-Dalipi, Z. The Association between Periodontal Disease and Preterm Low Birthweight in Kosovo. Acta Stomatol. Croat. 2017, 51, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Jaiman, G.; Nayak, P.A.; Sharma, S.; Nagpal, K. Maternal periodontal disease and preeclampsia in Jaipur population. J. Indian Soc. Periodontol. 2018, 22, 50–54. [Google Scholar]
- Boggess, K.A. Maternal Oral Health in Pregnancy. Obstet. Gynecol. 2008, 111, 976–986. [Google Scholar] [CrossRef]
- Puertas, A.; Magan-Fernandez, A.; Blanc, V.; Revelles, L.; O’Valle, F.; Pozo, E.; León, R.; Mesa, F. Association of periodontitis with preterm birth and low birth weight: A comprehensive review. J. Matern.-Fetal Neonatal Med. 2018, 31, 597–602. [Google Scholar] [CrossRef]
- Codato, L.A.B.; Nakama, L.; Cordoni Júnior, L.; Higasi, M.S. Atenção odontológica à gestante: Papel dos profissionais de saúde. Ciênc. Saúde Coletiva 2011, 16, 2297–2301. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oral Health Care During Pregnancy Expert Workgroup. Oral Health Care During Pregnancy: A National Consensus Statement; National Maternal and Child Oral Health Resource Center: Washington, DC, USA, 2012.
- Wilder, R.S. Is Dentistry at Risk? A Case for Interprofessional Education. J. Dent. Educ. 2008, 72, 1231–1237. [Google Scholar] [PubMed]
- Da Rocha, J.M.; Chaves, V.R.; Urbanetz, A.A.; Baldissera, R.D.S.; Rösing, C.K. Obstetricians’ knowledge of periodontal disease as a potential risk factor for preterm delivery and low birth weight. Braz. Oral Res. 2011, 25, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Alves, R.T.; Ribeiro, R.A.; Costa, L.R.; Leles, C.R.; Freire, M.C.M.; Paiva, S.M. Oral Care during Pregnancy: Attitudes of Brazilian Public Health Professionals. Int. J. Environ. Res. Public Health 2012, 9, 3454–3464. [Google Scholar] [CrossRef]
- Wilder, R.; Robinson, C.; Jared, H.L.; Boggess, K. Obstetricians’ Knowledge and Practice Behaviors Concerning Periodontal Health and Preterm Delivery and Low Birth Weight. J. Dent. Hyg. 2007, 81, 1–15. [Google Scholar]
- Cohen, L.; Schaeffer, M.; Davideau, J.-L.; Tenenbaum, H.; Huck, O. Obstetric Knowledge, Attitude, and Behavior Concerning Periodontal Diseases and Treatment Needs in Pregnancy: Influencing Factors in France. J. Periodontol. 2015, 86, 398–405. [Google Scholar] [CrossRef]
- Lim, M.; Riggs, E.; Shankumar, R.; Marwaha, P.; Kilpatrick, N. Midwives’ and women’s views on accessing dental care during pregnancy: An Australian qualitative study. Aust. Dent. J. 2018, 63, 320–328. [Google Scholar] [CrossRef]
- Wooten, K.T.; Lee, J.; Boggess, K.; Jared, H.; Wilder, R.S. Nurse Practitioner’s and Certified Nurse Midwives’ Knowledge, Opinions and Practice Behaviors regarding Periodontal Disease and Adverse Pregnancy Outcomes. J. Dent. Hyg. 2011, 85, 122–131. [Google Scholar]
- George, A.; Dahlen, H.G.; Reath, J.; Ajwani, S.; Bhole, S.; Korda, A.; Chok, H.N.; Miranda, C.; Villarosa, A.; Johnson, M. What do antenatal care providers understand and do about oral health care during pregnancy: A cross-sectional survey in New South Wales, Australia. BMC Pregnancy Childbirth 2016, 16, 382. [Google Scholar] [CrossRef] [Green Version]
- De Oliveira Diniz, L.V.; da Costa, C.H.M.; Oliveira, A.F.B.; Forte, F.D.S. Health professionals’ knowledge of oral health preventive practices regarding early childhood health care. J. Public Health 2012, 20, 513–518. [Google Scholar] [CrossRef]
- George, A.; Johnson, M.; Duff, M.; Ajwani, S.; Bhole, S.; Blinkhorn, A.; Ellis, S. Midwives and oral health care during pregnancy: Perceptions of pregnant women in south-western Sydney, Australia: Oral health care during pregnancy. J. Clin. Nurs. 2012, 21, 1087–1096. [Google Scholar] [CrossRef] [PubMed]
- Strafford, K.E.; Shellhaas, C.; Hade, E.M. Provider and patient perceptions about dental care during pregnancy. J. Matern.-Fetal Neonatal Med. 2008, 21, 63–71. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Ajwani, S.; Bhole, S.; Dahlen, H.; Reath, J.; Korda, A.; Ng Chok, H.; Miranda, C.; Villarosa, A.; Johnson, M. Knowledge, attitude and practises of dentists towards oral health care during pregnancy: A cross sectional survey in New South Wales, Australia. Aust. Dent. J. 2017, 62, 301–310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, A.; Ajwani, S.; Johnson, M.; Dahlen, H.; Blinkhorn, A.; Bhole, S.; Ellis, S.; Zheng, C.; Dawes, W. Developing and Testing of an Oral Health Screening Tool for Midwives to Assess Pregnant Woman. Health Care Women Int. 2015, 36, 1160–1174. [Google Scholar] [CrossRef]
- Bhole, S.; Ajwani, S.; George, A.; Johnson, M.; Blinkhorn, A.; Ellis, S. Oral health care model for pregnant women in Southwest Sydney. In Proceedings of the 88th International Association of Dental Research General Session, Barcelona, Spain, 14–17 July 2010. Journal of Dental Research: Volume 89, Abstract no. 138958. [Google Scholar]
- George, A.; Johnson, M.; Blinkhorn, A.; Ajwani, S.; Ellis, S.; Bhole, S. Views of pregnant women in South Western Sydney towards dental care and an oral-health program initiated by midwives. Health Promot. J. Aust. 2013, 24, 178–184. [Google Scholar] [CrossRef]
- Keirse, M.J.N.C.; Plutzer, K. Women’s attitudes to and perceptions of oral health and dental care during pregnancy. J. Perinatal Med. 2010, 38. [Google Scholar] [CrossRef] [Green Version]
- George, A.; Lang, G.; Johnson, M.; Ridge, A.; de Silva, A.M.; Ajwani, S.; Bhole, S.; Blinkhorn, A.; Dahlen, H.G.; Ellis, S.; et al. The evaluation of an oral health education program for midwives in Australia. Women Birth 2016, 29, 208–213. [Google Scholar] [CrossRef]
- Batchelor, P. Is periodontal disease a public health problem? Br. Dent. J. 2014, 217, 405–409. [Google Scholar] [CrossRef] [Green Version]
- Kaufman, L.B.; Henshaw, M.M.; Brown, B.P.; Calabrese, J.M. Oral Health and Interprofessional Collaborative Practice. Dent. Clin. N. Am. 2016, 60, 879–890. [Google Scholar] [CrossRef]
- Mortensen, B.; Lieng, M.; Diep, L.M.; Lukasse, M.; Atieh, K.; Fosse, E. Improving Maternal and Neonatal Health by a Midwife-led Continuity Model of Care—An Observational Study in One Governmental Hospital in Palestine. EClinicalMedicine 2019, 10, 84–91. [Google Scholar] [CrossRef] [Green Version]
- Sandall, J.; Soltani, H.; Gates, S.; Shennan, A.; Devane, D. Midwife-led continuity models versus other models of care for childbearing women. Cochrane Database Syst. Rev. 2016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Homer, C.S. Models of maternity care: Evidence for midwifery continuity of care. Med. J. Aust. 2016, 205, 370–374. [Google Scholar] [CrossRef] [PubMed]
- Dahlen, H.G.; Johnson, M.; Hoolsema, J.; Norrie, T.P.; Ajwani, S.; Blinkhorn, A.; Bhole, S.; Ellis, S.; Srinivas, R.; Yaacoub, A.; et al. Process evaluation of the midwifery initiated oral health-dental service program: Perceptions of midwives in Greater Western Sydney, Australia. Women Birth 2019, 32, 159–165. [Google Scholar] [CrossRef] [PubMed]
- George, A.; Villarosa, A.; Patterson Norrie, T.; Hoolsema, J.; Dahlen, H.; Ajwani, S.; Bhole, S.; Blinkhorn, A.; Srinivas, R.; Yaacoub, A.; et al. Process evaluation of the midwifery initiated oral health-dental service program: Perceptions of pregnant women. Aust. Dent. J. 2019, 64, 55–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Maternal and Child Oral Health Resource Center. Oral Health Care During Pregnancy: A Resource Guide, 2nd ed.; National Maternal and Child Oral Health Resource Center: Washington, DC, USA, 2017. [Google Scholar]
- Sanz, M.; Kornman, K. Periodontitis and adverse pregnancy outcomes: Consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Clin. Periodontol. 2013, 40, 164–169. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NHS Inform. Looking After Your Teeth and Gums in Pregnancy; NHS Health Scotland: Edinburgh, Scotland, 2019; Available online: https://www.nhsinform.scot/ready-steady-baby/pregnancy/looking-after-yourself-and-your-baby/looking-after-your-teeth-and-gums-in-pregnancy (accessed on 18 February 2020).
- Australian Health Ministers’ Advisory Council. Clinical Practice Guidelines: Antenatal Care—Module 1; Australian Government Department of Health and Ageing: Canberra, ACT, Australia, 2012.
- Australian Government Department of Health. Clinical Practice Guidelines: Pregnancy Care; Australian Government Department of Health: Canberra, ACT, Australia, 2018.
- Duff, M.; Dahlen, H.G.; Burns, E.; Priddis, H.; Schmied, V.; George, A. Designing an oral health module for the Bachelor of Midwifery program at an Australian University. Nurse Educ. Pr. 2017, 23, 76–81. [Google Scholar] [CrossRef]
- Midwife Accreditation Standards 2014; Australian Nursing and Midwifery Accreditation Council: Canberra, ACT, Australia, 2014; ISBN 978-0-9808210-6-2. Available online: https://www.anmac.org.au/sites/default/files/documents/ANMAC_Midwife_Accreditation_Standards_2014.pdf (accessed on 20 May 2019).
- Nursing and Midwifery Board of Australia. Midwife Standards for Practice; Nursing and Midwifery Board AHPRA: Canberra, ACT, Australia, 2018. Available online: https://www.nursingmidwiferyboard.gov.au/Codes-Guidelines-Statements/Professional-standards/Midwife-standards-for-practice.aspx (accessed on 20 May 2019).
- Internet, Phone, Mail, and Mixed-Mode Surveys: The Tailored Design Method, 4th ed.; Dillman, D.A.; Smyth, J.D.; Christian, L.M. (Eds.) Wiley: Hoboken, NJ, USA, 2014; ISBN 978-1-118-45614-9. [Google Scholar]
- Peterson, R. Constructing Effective Questionnaires; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2000; ISBN 978-0-7619-1641-3. [Google Scholar]
- Handbook of Health Research Methods: Investigation, Measurement and Analysis; Bowling, A. (Ed.) Reprinted; Open Univ. Press: Maidenhead, UK, 2009; ISBN 978-0-335-21460-0. [Google Scholar]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 2009, 42, 377–381. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inform. 2019, 95, 103208. [Google Scholar] [CrossRef]
- Health Practitioner Regulation National Law 2018 (ACT), Republication No 9; ACT Parliamentary Counsel: Canberra, ACT, Australia, 2019. Available online: http://www.legislation.act.gov.au/a/db_39269/current/pdf/db_39269.pdf (accessed on 21 May 2019).
- Australian Institute of Health and Welfare. Nursing and Midwifery Workforce 2015; Australian Institute of Health and Welfare: Canberra, ACT, Australia, 2016.
- Heilbrunn-Lang, A.Y.; de Silva, A.M.; Lang, G.; George, A.; Ridge, A.; Johnson, M.; Bhole, S.; Gilmour, C. Midwives’ perspectives of their ability to promote the oral health of pregnant women in Victoria, Australia. BMC Pregnancy Childbirth 2015, 15, 110. [Google Scholar] [CrossRef] [Green Version]
- Catford, J. Turn, turn, turn: Time to reorient health services. Health Promot. Int. 2014, 29, 1–4. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| % | n | ||
|---|---|---|---|
| Gender | Female | 100.0% | 100 |
| Male | 0.0% | 0 | |
| Other | 0.0% | 0 | |
| Number of years in midwifery practice | Current midwifery student | 32.0% | 32 |
| Less than 10 years | 44.0% | 44 | |
| 10–20 years | 11.0% | 11 | |
| 21–30 years | 10.0% | 10 | |
| 31–40 years | 6.0% | 6 | |
| 40+ years | 0.0% | 0 | |
| Current occupation | Currently practicing midwife in Australia | 68.0% | 68 |
| Current midwifery student | 32.0% | 32 | |
| Unemployed | 0.0% | 0 | |
| Retired midwife | 0.0% | 0 | |
| Midwifery practice location | Urban | 77.0% | 77 |
| Rural | 23.0% | 23 | |
| Midwifery practice setting | Hospital | 85.0% | 85 |
| Hospital and private practice | 13.0% | 13 | |
| Private practice | 2.0% | 2 | |
| How would you rate your oral health? | Excellent | 22.0% | 22 |
| Good | 58.0% | 58 | |
| Neutral | 14.0% | 14 | |
| Poor | 6.0% | 6 | |
| Very poor | 0.0% | 0 | |
| How often do you visit the dentist? | Every 6 months | 33.0% | 33 |
| Every 12 months | 33.0% | 33 | |
| Every 12-18 months | 21.0% | 21 | |
| Only if in pain | 12.0% | 12 | |
| Never | 1.0% | 1 | |
| Have you ever been diagnosed with periodontal disease? | Yes | 23.0% | 23 |
| No | 77.0% | 77 | |
| Have you ever been diagnosed and received treatment for periodontal disease? | Yes | 22.0% | 22 |
| No | 78.0% | 78 |
| Survey Question | Respondent Answer | % | n |
|---|---|---|---|
| Definition of periodontal disease (N = 154) | Inflammation and bacterial infection | 63.0% | 97 |
| Degenerative process | 31.8% | 49 | |
| Auto-immune disorder | 2.0% | 3 | |
| Osteoporosis | 2.0% | 3 | |
| Metastatic process | 1.3% | 2 | |
| Clinical signs associated with periodontal disease (N = 343) | Gingival bleeding | 28.9% | 99 |
| Tooth mobility | 21.6% | 74 | |
| Tooth loss | 21.0% | 72 | |
| Caries | 16.0% | 55 | |
| Alveolar bone destruction | 12.5% | 43 | |
| Risk factors for gum disease initiation (N = 409) | Poor oral hygiene | 23.5% | 96 |
| Smoking | 20.0% | 82 | |
| Excessive sugar consumption | 14.7% | 60 | |
| Tooth decay | 10.0% | 41 | |
| Dental plaque | 14.2% | 58 | |
| Genetics | 9.0% | 37 | |
| Pregnancy | 8.6% | 35 | |
| Risk factors for gum disease progression (N = 396) | Poor oral hygiene | 23.5% | 93 |
| Smoking | 18.2% | 72 | |
| Excessive sugar consumption | 16.4% | 65 | |
| Tooth decay | 11.6% | 46 | |
| Dental plaque | 15.9% | 63 | |
| Genetics | 3.0% | 12 | |
| Pregnancy | 11.4% | 45 | |
| Oral signs often related to pregnancy (N = 162) | Gingival bleeding | 61.1% | 99 |
| Gingival overgrowth | 20.4% | 33 | |
| Caries | 9.3% | 15 | |
| Tooth loss | 9.3% | 15 | |
| Do periodontal diseases influence pregnancy outcomes? (N = 192) | Yes – Increased incidence of preterm birth | 34.9% | 67 |
| Yes – Increased incidence of low-weight newborn | 20.3% | 39 | |
| Yes – Increased incidence of spontaneous abortion | 17.7% | 34 | |
| Yes – Increased incidence of low genital-tract infection | 10.4% | 20 | |
| Yes – increased incidence of pre-eclampsia | 7.8% | 15 | |
| No | 8.9% | 17 | |
| Are periodontal diseases preventable during pregnancy? (N = 100) | Yes – They can be prevented or arrested during pregnancy | 98.0% | 98 |
| No – They’re an expected side effect during pregnancy | 2.0% | 2 | |
| Periodontal diseases can be prevented by: (N = 382) | Effective toothbrushing technique | 25.4% | 97 |
| Using dental floss or interdental brushes | 25.1% | 96 | |
| Smoking cessation | 22.5% | 86 | |
| Using fluoridated toothpaste | 19.1% | 73 | |
| Control of psychological stress | 7.9% | 30 |
| Likert-Scale Questions | Strongly Agree %(N) | Agree % (N) | Neutral % (N) | Disagree % (N) | Strongly Disagree % (N) |
|---|---|---|---|---|---|
| For patients with periodontal disease, periodontal treatment is beneficial for improving oral health | 82.0%(82) | 18.0%(18) | 0%(0) | 0%(0) | 0%(0) |
| Periodontal disease can have an adverse effect on pregnancy outcomes | 41.0%(41) | 40.0%(40) | 11.0%(11) | 8.0%(8) | 0%(0) |
| Treatment of periodontal disease during pregnancy positively affects pregnancy outcomes | 38.0%(38) | 42.0%(42) | 17.0%(17) | 2.0%(2) | 1.0%(1) |
| Asking pregnant patients about their oral health is outside the routine practices of a midwife | 9.0%(9) | 16.0%(16) | 6.0%(6) | 34.0%(34) | 35.0%(35) |
| Conducting an examination of the oral cavity during pregnancy is outside the routine practices of a midwife | 41.0%(41) | 40.0%(40) | 5.0%(5) | 10.0%(10) | 4.0%(4) |
| It is important for a pregnant woman to receive routine dental care during her pregnancy | 57.0%(57) | 37.0%(37) | 5.0%(5) | 1.0%(1) | 0%(0) |
| There is not sufficient time to address oral health during a care visit with a midwife | 16.0%(16) | 26.0%(26) | 18.0%(18) | 33.0%(33) | 7.0%(7) |
| I am up to date on the topic of oral health and pregnancy | 3.0%(3) | 13.0%(13) | 28.0%(28) | 42.0%(42) | 14.0%(14) |
| Additional questions | % (N) | ||||
| I routinely ask questions related to oral health during consultation with pregnant patients | Yes | 60.0%(60) | |||
| No | 40.0%(40) | ||||
| I routinely perform a visual oral examination during consultation with pregnant patients | Yes | 7.0%(7) | |||
| No | 93.0%(93) | ||||
| I provide oral-health-related information during consultation with pregnant patients | Routinely | 39.0%(39) | |||
| If patient is considered at risk | 40.0%(40) | ||||
| Never | 21.0%(21) | ||||
| I refer patients to their dentist for a check-up | Routinely | 49.0%(49) | |||
| If patient is considered at risk | 33.0%(33) | ||||
| Never | 18.0%(18) | ||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, J.G.-l.; Nanayakkara, S.; Holden, A.C.L. Knowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant Patients. Int. J. Environ. Res. Public Health 2020, 17, 2246. https://doi.org/10.3390/ijerph17072246
Nguyen JG-l, Nanayakkara S, Holden ACL. Knowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant Patients. International Journal of Environmental Research and Public Health. 2020; 17(7):2246. https://doi.org/10.3390/ijerph17072246
Chicago/Turabian StyleNguyen, Jennifer Gia-linh, Shanika Nanayakkara, and Alexander C. L. Holden. 2020. "Knowledge, Attitudes and Practice Behaviour of Midwives Concerning Periodontal Health of Pregnant Patients" International Journal of Environmental Research and Public Health 17, no. 7: 2246. https://doi.org/10.3390/ijerph17072246